
More Information
Submitted: July 14, 2023 | Approved: July 22, 2023 | Published: July 25, 2023
How to cite this article: Marzouq MK, Ismail KA, Mahmoud AM, Khalifa OM. Case Report of Gardner-Diamond Syndrome. Ann Dermatol Res. 2023; 7: 028-031.
DOI: 10.29328/journal.adr.1001027
Copyright License: © 2023 Marzouq MK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Gardner-diamond syndrome; Depression; Purpura

Case Report of Gardner-Diamond Syndrome
Mahmoud K Marzouq1, Khadiga A Ismail2*, Ahmed M Mahmoud3 and Osama M Khalifa4
1Consultant of Dermatology and Venereology, King Faisal Medical Complex, Taif, KSA
2Department of Medical Parasitology, Faculty of Medicine, Ain Shams University, Cairo, Egypt
3Department of Urology, Mayo Clinic, Rochester, MN, USA
4Department of Internal Medicine, Faculty of Medicine, Ain Shams University, Cairo, Egypt
*Address for Correspondence: Khadiga A Ismail, Department of Medical Parasitology, Faculty of Medicine, Ain Shams University, Cairo, Egypt, Email: [email protected]
Gardner-Diamond syndrome or psychogenic purpura is a rare vasculopathy disorder characterized by spontaneous painful purpuric rash without a history of trauma or antiplatelet or anticoagulant therapy. It occurs in women with mental health disorders. Gardner and Diamond in 1955 described a syndrome of auto erythrocyte sensitization which presented in abnormal crops of painful inflammatory ecchymosis in 4 patients at the site of trauma followed by progressive erythema and edema.
We present a 52-year-old age woman who was admitted to the internal medicine department and referred for dermatological consultation for recurrent spontaneous purpuric eruptions. The patient was under treatment for depression for many months. Her investigations and coagulation profile were nearly within normal.
52 years female patient, presented with acute onset on top of intermittent courses of purpuric rash. The rash was not associated with fever, fatigue, loss of appetite, loss of weight, or hematuria. The rash was mild in distribution and severity in the last 8 months, but it is severe for a few days. The rash was distributed in the face, front of the chest, and less in the lower extremities. Some lesions are painful. There was no bleeding from any orifices. She has no history of previous thrombosis or abortion. She has a past history of oral ulcers, hair loss, recurrent abdominal pain, recurrent headache, and bone pain. She was under treatment for diabetes with metformin 500 mg TID and sitagliptin 100 mg once daily, treatment of depression with duloxetine 60 mg once daily, treatment of abdominal pain with mebeverine 200 mg bid, and treatment of hypertension with perindopril 5 mg once daily, and paracetamol for recurrent headache since many years.
On examination
The patient was afebrile, alert, and oriented. Her temperature was 37.1 °C, her blood pressure was 118/78 mm Hg with a heart rate of 75 beats/minute, respiratory rate of 16 breaths/minute, and oxygen saturation of 94% in room temperature air.
Her neck was soft, and easily mobile without lymphadenopathy or mass. Her heart had a regular rate and rhythm without murmur. Her lungs were clear to auscultation bilaterally. The abdominal exam showed a soft, non-distended abdomen without tenderness. There was no oral ulcer.
The skin examination showed Generalized deep ecchymotic lesions on the forehead, both upper extremities, and less in the lower extremities, some of the lesions were painful and tender in Figures 1-3.

Figure 1: Showed a purpuric rash on the dorsal surface of the left forearm with hypopigmented maculopatches lesions.

Figure 2: Showed a purpuric rash with hypopigmented maculopatches lesions over the dorsum surface of the left hand.
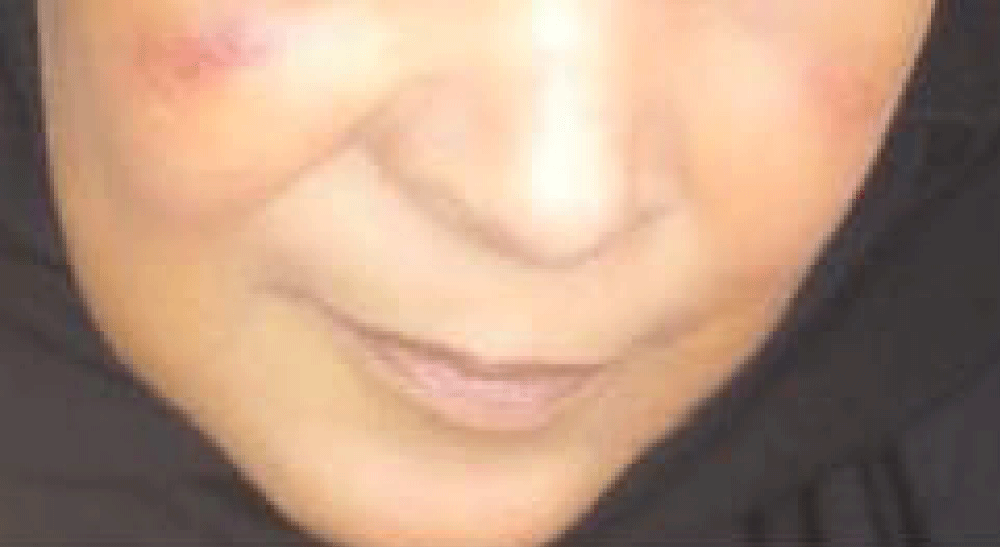
Figure 3: Showed a faint purpuric rash on both cheeks. This figure was taken in the dermatology clinic after discharge from the hospital.
She had reported previous episodes of mild bruising in the face and lower extremities without trauma, or use of antiplatelet and anticoagulants such as aspirin.
The clinically significant results are as follows
White blood cell count (WBC) of 4.97 k/µL (N) (normal 4 – 10 k/µL), with lymphocytosis (48.50%) (normal 20% - 40%), low neutrophils (38.60%) (normal 40% - 80%), normal platelets (238) (normal 150–410), Red blood cell count (RBC) of 4.18 M/µL (L) (normal 4.5 - 5.5 M/µL) with hemoglobin of 10.70 g/dL (L) (normal 12-15g/dL), and hematocrit of 32.90% (L) (normal 36% - 46%).
As regard her chemistry: Her random glucose of 89.90 mg/dL (N) (normal 70-140 mg/dL), blood urea of 16.30 mg/dL (L) (normal 20-48 mg/dL), creatinine of 0.87 mg/dL (N) (normal 0.5-1.1 mg/dL), normal liver function tests, and normal LDH (198 uL) (normal 135-214 uL).
As regards the coagulation profile: Partial thromboplastin time (PTT) was (34.40 sec.) (N) (normal 26-40 seconds), thromboplastin time (PT) of (13.60 sec.) (N) (normal 11-14.5 seconds), and INR of 1.1 % (N) (normal 0.8% - 1.2%).
As regard clotting profile, CRP (C-reactive protein), thyroid profile (T3, T4 and TSH), RF (rheumatoid factor), and ANA (antinuclear antibodies) were within normal.
Ultrasound of the abdomen showed: Mild hepatomegaly with fatty changes and rest scan appears unremarkable.
MRI Brain with contrast showed: Unremarkable MRI study of the brain, and partial empty sella.
The diagnosis of auto erythrocyte sensitization syndrome (psychogenic purpura) was suspected according to these abnormal patterns of ecchymosis, the associated pain and tender in some of the ecchymotic lesions, the normal laboratory results especially the normal coagulation profile, and the history of depression illness.
Gardner-Diamond syndrome (GDS) or psychogenic purpura was prescribed in the early 20th century by the German psychiatrist Rudolf Schindler. He described 16 patients with skin hemorrhages. A few years later in 1928, Shustik C. described 2 other cases of purpura which was associated with psychiatric illness as delusions, and hysterical personality, thereby, connecting the skin lesions.
In 1955, Gardner and Diamond described 4 women cases who had painful ecchymoses at the site of trauma followed by progressive erythema and edema. The auto-sensitization of patients to their own blood was described as “Gardner-Diamond syndrome” [1].
In 1989, Oscar D. Ratnoff reported a series of 71 cases of auto erythrocyte sensitization syndrome. He described them as the term “psychogenic purpura” [2].
The link between psychological disturbances and developing this psychological purpura is not clear well. The psychological stress may be associated with the psycho-endocrine model, thereby, neuropeptide signaling molecules expressed and released by neurons act upon cell surface receptors, ultimately leading to an alteration of hemostatic physiologic processes via catecholamine and glucocorticoid release [3,4]. Besides to neuroendocrine axis, there are other factors related to the pathogenesis of psychogenic purpura such as immunologic, hematologic, hormonal, vascular, and subjacent inflammatory conditions [5.6].
Gardner-Diamond syndrome (GDS) or psychogenic purpura is known also as auto erythrocyte sensitization syndrome. Stress causes auto-sensitization to phosphatidylserine, a component of the erythrocyte stroma. Phosphatidylserine has an atypical cellular organization in GDS [7,8]. Stress can cause alterations in the composition of erythrocyte membrane phospholipids [9].
GDS is typically seen mainly in adult females, and occasionally seen in the male and children [1]. Psychogenic purpura is associated with patients with a variety of psychological diseases such as depression, anxiety, obsessive-compulsive disorders, sexual problems, feelings of hostility, and borderline personality disorders [1,2].
Skin symptoms are preceded by general discomfort and fatigue [10].
Psychogenic purpura may be associated with systemic symptoms such as headache, nausea, vomiting, abdominal pain, joint pain, and external hemorrhages such as epistaxis, gastrointestinal bleeding, and bleeding from ear canals [8,11].
Ecchymosis may occur simultaneously in several areas, especially on the limbs [12].
Pain and pruritus in the skin area where lesions will develop. Four to five hours later, a skin induration may be developed. Within one to two days, this skin induration turns into a painful ecchymotic patch, 3-10 cm in diameter. One to two weeks later, the lesion starts discoloring until it turns yellowish before finally fading leaving no scars [13].
Symptoms of GDS are exacerbated by exposure to copper [14].
Clinical pictures of GDS are usually benign and its prognosis is good; but some cases are associated with membranous glomerulopathy [15].
Differential diagnosis
1. Differential diagnosis of psychogenic purpura includes among other coagulopathies conditions which are related to bleeding disorders such as:Idiopathic thrombocytopenic purpura (ITP)
2. Henoch Schoenlein purpura
3. Systemic erythematous lupus (SLE)
4. Ehlers-Danlos Syndrome
5. Compartment syndrome
6. Weber-Christian panniculitis
7. Munchausen disease [16]
8. Some coagulation disorders such as acquired VIII factor inhibitor, hemophilic pseudo-tumor, and skin necrosis related to cumarinics [17].
Treatment
There are some medications that are tried to improve symptoms of psychogenic purpura such as glucocorticoids, pain medications, and hormonal contraceptives, but they are ineffective. Jafferany, et al. 2015 [8] also said that relief of acute stress and treatment of psychological factors is important for remission. Hypnosis and psychotherapy are effective in improving skin lesions in young patients [17].
Antidepressants, busulfan, and promethazine are used in the treatment of Gardner-Diamond syndrome [18,19]. Early diagnosis with early psychiatric therapy is most effective in the management of GDS [20-22].
Psychogenic purpura or Gardner-Diamond syndrome is known as auto erythrocyte sensitization syndrome. It is confusing with a lot of other purpuras, so we must differentiate it promptly from other similar diseases such as idiopathic thrombocytopenic purpura (ITP), HenochSchoenlein purpura, systemic erythematous lupus (SLE), etc. Early diagnosis of psychogenic purpura with early psychiatric therapy is beneficial to avoid misdiagnosis, delay management, mistreatment, and decreasing cost.
Ethical considerations: This case report was approved by the patient to be published.
- GARDNER FH, DIAMOND LK. Autoerythrocyte sensitization; a form of purpura producing painful bruising following autosensitization to red blood cells in certain women. Blood. 1955 Jul;10(7):675-90. PMID: 14389381.
- Ratnoff OD. Psychogenic purpura (autoerythrocyte sensitization): an unsolved dilemma. Am J Med. 1989 Sep;87(3N):16N-21N. PMID: 2486528.
- Panconesi E, Hautmann G. Stress, stigmatization and psychosomatic purpuras. Int Angiol. 1995 Jun;14(2):130-7. PMID: 8609439.
- Mason JW. The scope of psychoendocrine research. Psychosom Med. 1968 Sep-Oct;30(5):Suppl:565-75. doi: 10.1097/00006842-196809000-00019. PMID: 4975168.
- Baek JO, Jee HJ, Kim TK, Lee MG. Case of Gardner-Diamond syndrome after intramuscular stimulation. J Dermatol. 2011 Dec;38(12):1197-9. doi: 10.1111/j.1346-8138.2011.01232.x. Epub 2011 Jul 7. PMID: 21736604.
- Kalden JR, Höffken B, Stangel W. Immune mechanism in gardner-diamond syndrome. N Engl J Med. 1977 Dec 15;297(24):1350. doi: 10.1056/nejm197712152972413. PMID: 917094.
- Ivanov OL, Lvov AN, Michenko AV, Künzel J, Mayser P, Gieler U. Autoerythrocyte sensitization syndrome (Gardner-Diamond syndrome): review of the literature. J Eur Acad Dermatol Venereol. 2009 May;23(5):499-504. doi: 10.1111/j.1468-3083.2009.03096.x. Epub 2009 Feb 2. PMID: 19192020.
- Jafferany M, Bhattacharya G. Psychogenic Purpura (Gardner-Diamond Syndrome). Prim Care Companion CNS Disord. 2015 Jan 22;17(1):10.4088/PCC.14br01697. doi: 10.4088/PCC.14br01697. PMID: 26137346; PMCID: PMC4468873.
- Ponizovsky AM, Modai I, Nechamkin Y, Barshtein G, Ritsner MS, Yedgar S, Lecht S, Bergelson LD. Phospholipid patterns of erythrocytes in schizophrenia: relationships to symptomatology. Schizophr Res. 2001 Oct 1;52(1-2):121-6. doi: 10.1016/s0920-9964(00)00189-4. PMID: 11595399.
- Silny W, Marciniak A, Czarnecka-Operacz M, Zaba R, Schwartz RA. Gardner-Diamond syndrome. Int J Dermatol. 2010 Oct;49(10):1178-81. doi: 10.1111/j.1365-4632.2009.04396.x. PMID: 20883407.
- Meeder R, Bannister S. Gardner-Diamond syndrome: Difficulties in the management of patients with unexplained medical symptoms. Paediatr Child Health. 2006 Sep;11(7):416-9. doi: 10.1093/pch/11.7.416. PMID: 19030312; PMCID: PMC2528627.
- National Institutes of Health. Gardner-Diamond Syndrome. 2016. https://rarediseases.info.nih.gov/diseases/6481/gardner-diamond-syndrome.
- Harth W, Taube KM, Gieler U. Facticious disorders in dermatology. J Dtsch Dermatol Ges. 2010 May;8(5):361-72; quiz 373. English, German. doi: 10.1111/j.1610-0387.2010.07327.x. Epub 2010 Feb 12. PMID: 20163503.
- Grossman RA. Autoerythrocyte sensitization worsened by a copper-containing IUD. Obstet Gynecol. 1987 Sep;70(3 Pt 2):526-8. PMID: 3627621.
- Jefferson JA, Nelson PJ, Najafian B, Shankland SJ. Podocyte disorders: Core Curriculum 2011. Am J Kidney Dis. 2011 Oct;58(4):666-77. doi: 10.1053/j.ajkd.2011.05.032. Epub 2011 Aug 24. PMID: 21868143; PMCID: PMC3183322.
- Tomec RJ, Walsh M, Garcia JC, Jordan PK. Diagnosis of autoerythrocyte sensitization syndrome in the emergency department. Ann Emerg Med. 1989 Jul;18(7):780-2. doi: 10.1016/s0196-0644(89)80019-8. PMID: 2735600.
- Bartralot R, González-Castro U, Repiso T, Castells Rodellas A. Autoerythrocyte sensitization syndrome (psychogenic purpura)]. Clinical Medicine. 1995; 105(3): 117–118.
- Gomi H, Miura T. Autoerythrocyte sensitization syndrome with thrombocytosis. Dermatology. 1994;188(2):160-2. doi: 10.1159/000247125. PMID: 8136547.
- Vun YY, Muir J. Periodic painful purpura: fact or factitious? Australas J Dermatol. 2004 Feb;45(1):58-63. doi: 10.1111/j.1440-0960.2004.00049.x. PMID: 14961912.
- Sorensen RU, Newman AJ, Gordon EM. Psychogenic purpura in adolescent patients. Clin Pediatr (Phila). 1985 Dec;24(12):700-4. doi: 10.1177/000992288502401206. PMID: 4064457.
- Schindler R. Nervous system and spontaneous bleeding. S Karger, Berlin, Germany 1927.
- Shustik C. Gardner-Diamond's syndrome in a man. Arch Intern Med. 1977 Nov;137(11):1621-2. PMID: 921453.